
Learning that your child may need craniofacial surgery can be a stressful experience for parents. Craniofacial surgery is commonly performed on infants and children who have birth defects, trauma, or other medical conditions that impact the head and face. Surgical interventions often focus on reconstruction to enable normal growth, development, and function for the child while also improving appearance. Our surgeons work with your family and child to develop an optimal plan of care, ensuring the best possible outcome for your child.
Craniosynostosis
When babies are first born, their skull bones are still in the process of developing. A typical newborn’s skull comprises of multiple bones separated by flexible and fibrous joints called sutures. This flexibility allows the bony plates to move as the skull continues to expand, accommodating for brain growth. As the newborn continues to mature, the sutures eventually fuse together resulting in a more solid and continuous piece of bone.
Craniosynostosis is a common craniofacial anomaly in children. Approximately 1 in every 1500-1900 infants born each year in the United States is born with craniosynostosis. Although craniosynostosis may be related to an underlying condition, it most commonly occurs as a stand alone "single suture fusion." Infants with abnormal head shapes are identified at or soon after birth, and they are optimally cared for in a multidisciplinary care setting. Depending on the severity of the craniosynostosis, the condition if left untreated can cause developmental delays or vision impairment. Early evaluation, diagnosis, and treatment planning tends to lead to very good outcomes.
Sutures are soft fibrous seams that separate the plates of bones in an infant’s skull. As the infant matures, these sutures allow the bony plates to move and expand to accommodate the brain as it continues to grow.
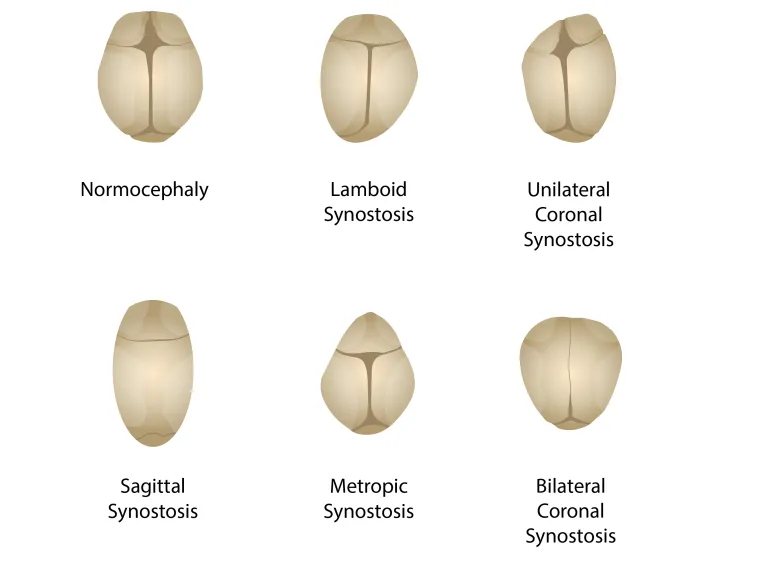
Sometimes, one or more of these sutures that separate the plates of the skull close too early, which is called craniosynostosis. This prevents the skull from growing normally in all directions, which may lead to an abnormal shape. The shape of the skull of an infant with craniosynostosis depends on the suture that has closed. For example, a long and narrow head shape may occur when the central midline suture (the sagittal suture) closes too early. In that case, the skull is unable to grow side to side, leading to overgrowth from the front to back. Most often, a single suture closes too early, though it is possible for more than one to be involved.
It is unknown why craniosynostosis occurs. Many babies affected by craniosynostosis typically have one suture involved with no other health problems.
Alternatively, craniosynostosis can occur as part of a genetic syndrome like Crouzon, Apert, Pfeiffer, or Saethre-Chotzen. Commonly, there is more than one suture involved in these children, and these syndromes may be passed on in families between multiple generations. You may be aware of relatives who share the same condition. Your doctors can advise you if genetic testing is recommended for your child
For minor cases that do not require surgical intervention, helmet therapy, also known as cranial orthosis, may be used to gradually correct your baby’s skull in a less invasive way. The helmet is specially made for your child with a hard outer shell and a softer foam lining creating consistent pressure on the skull to promote natural skull growth. Though the helmet must be worn for the majority of the day, helmet therapy should not be painful or uncomfortable for your child. Duration of this treatment is about three months on average, but it can vary depending on your child’s condition and age.
For cases where the head is misshapen significantly, treatment usually involves surgery. Two surgical interventions are available to help treat craniosynostosis and adjust an infant’s head shape.
Endoscopic Strip Craniectomy: This surgery is performed on infants under 3 months of age with a fused sagittal (midline) sutures. During the surgical procedure, the surgeon creates two small incisions into the infant’s skull and uses a special camera to locate and visualize the fused sagittal suture. After locating the sutures, they are then cut out and removed. A helmet will be given to help promote reshaping of the skull. It is important to note that the infant’s skull continues to grow and does not reach full development until 18 months post-surgery.
Open Remodeling: This surgery is typically performed between 6-12 months of age. The surgeon first exposes the abnormal shaped skull bones through an ear to ear incision. The bones are then removed to be molded. During this age, the infant’s skull bones are still flexible enough to be reshaped with the surgeon's hands, but are strong enough to hold resorbable plates and screws. Unlike endoscopic strip craniectomy, this procedure creates complete normalization of the skull shape and does not require helmet therapy. However, this surgery is a longer process and has an increased risk of significant blood loss; pre-planned blood transfusions are utilized to prevent further complications. If necessary, blood transfusion can deliver platelets or clotting factors to prevent or treat bleeding disorders.
Surgical Treatment of Craniosynostosis
There are three reasons you doctor may recommend surgery to treat craniosynostosis:
- Cosmetically, surgical intervention helps normalize the shape of the babies’ skull. In some cases, without intervention, the shape of the skull will not improve and distortion may progress.
- Because the closed sutures limit the skull bones’ ability to grow in response to a developing brain, pressure inside the skull can build, eventually leading to neurologic problems. These are rare in cases of single suture craniosynostosis. Expanding the skull through surgical intervention treats or prevents this.
- There is an association between single suture craniosynostosis and developmental delays, especially in craniosynostosis of the metopic suture. Some evidence suggests that surgical treatment improves developmental outcomes.
You may wish to have the surgery performed as soon as your child receives a craniosynostosis diagnosis. However, the best time for surgery depends on which suture is involved and the baby’s overall health and development. Commonly, the surgery is performed during the infant’s first year while the skull bones are relatively soft and moldable. Your surgeons will discuss optimal timing for your baby's procedure. Most children need only one surgery.
Our multidisciplinary team will meet with you and your family to evaluate your infant. You will have one or more visits with our craniofacial team. Your baby’s evaluation will include a visit with a pediatric craniofacial surgeon, a pediatric neurosurgeon, a developmental pediatrician, a pediatric ophthalmologist, and possibly a genetic doctor. A CT scan of the head may be recommended. After your evaluations are complete, your baby’s team of providers will share their diagnosis and recommend a treatment plan.
After setting a surgical date, you will meet with a pediatric anesthesiologist to get blood work done on your infant if your infant is undergoing open remodeling surgery. Plans for blood donation and/or transfusion will be made as well. Blood can be obtained from a variety of sources including the parents, other family members, or the hospital’s blood bank or donation center. The blood that is used will match the infant's blood type. During this visit, your doctor will also advise you on when to stop food and liquids before surgery and what to bring with you to the hospital the day of surgery. If your child will need a postoperative helmet, you and your baby will also have a fitting session with an orthotist who will be developing your infant’s personalized helmet.
Your child will be admitted to the preoperative area early on the morning of surgery. You will meet with your anesthesiologist and surgeon for one last time. A nurse will show you where to wait during the surgery, and they will update you periodically during the procedure. After the surgery is completed, your surgeons will speak with you to give you a report on how the operation went. Your child will then be transferred into the Pediatric Intensive Care Unit (PICU) from the operating room. Once your child is checked into the PICU, you may visit with them.
Your child will be cared for in the PICU for the first one to two nights, and during that early post-operative time, your baby may experience a few expected reactions as they start their healing process.
For example, your infant may have forehead and eyelid swelling to the extent where sometimes the eyes swell shut. This usually occurs one to three days after surgery. Additionally, expect your child to have a fever within the first two days after surgery. During this time, the nurses will help you hold and comfort your child. Your child may have IVs to help administer pain medicines, as well as a drain exiting behind one ear and a bladder catheter. They will be on monitors to follow heart rate, blood pressure, and oxygen levels to ensure their recovery is going smoothly. Once fully awake from anesthesia, your infant will be offered liquids and will eventually be transitioned to oral medications. When the team feels your child is ready, they will be transferred to a regular floor room. Nurses on the floor ward will teach you how to care for your child’s incision and how to give them medicines in preparation for discharge to home.
Once home, your child will return to their previous schedule and habits of eating normally, sleeping normally, and playing again. Closely monitor your child for several months after surgery to assure they do not fall and hit the head. While the bone repair is very secure, significant force to the incision can reopen it.
Make an Appointment
For the best plastic and reconstructive surgical care in Tucson, Southern Arizona or the Southwest, make an appointment by calling
(520) 694-8888.
Contact Us
University of Arizona Department of Surgery
Section of Plastic and Reconstructive Surgery
1501 N. Campbell Ave.
Tucson, Arizona 85724
Office Phone: (520) 626-9383
Fax: (520) 441-4945